

December 1st, 2016 marked World AIDS Day. This year’s theme is “Leadership. Commitment. Impact.” The White House National HIV/AIDS Strategy for the United States praises the collective efforts of the healthcare workforce, including “increased access to new, sterile syringes and other injection equipment to minimize infections from injection drug use.”
Syringe services programs (SSPs) have proved beneficial to countries across the globe. In Hong Kong SAR, pharmacies can provide new syringes without a prescription. Surveys by the health department find that only 2% of HIV infections are attributable to persons who inject drugs (PWIDs) in this country. In Berlin, Germany, 77% of PWIDs use syringe vending machines at least 4 times per week. Elsewhere in Germany, syringe SSPs in jail dramatically reduce rate of new infections.
The evidence is clear: Syringe exchange programs work. Not only do they decrease HIV transmission among PWIDs, but they don’t recruit new drug users and they are cost-effective compared to treating individuals with HIV. So what’s the hold up? We need only look at the United States to see that legislation for SSPs is far from universal.

There are currently, 228 SSPs in 35 states, the District of Colombia, Puerto Rico, and the Indian Nations. In states without SSPs, the impact to PWIDs is devastating:
In jurisdictions in the United States, where drug paraphernalia laws were strictly enforced, higher prevalence of HIV infection was observed despite lower risk-taking behavior. Legal barriers in Maryland and Texas in the United States resulted in a high prevalence of HIV with up to 25% of PWIDs infected in Baltimore, Maryland and 35% of PWIDs infected in Houston, Texas. These findings overall suggest that injecting paraphernalia legislation that restricts needle and syringe availability inadvertently increases HIV infection. There is no convincing evidence that this legislation reduced HIV prevalence.
Whereas Maryland now has one SSPs, Texas is still one of 15 states that do not offer this service. This is especially concerning due to the prevalence of HIV on the US-Mexico border. Made possible by a combination of illegal and legal sex work, PWIDs, and the highly transient nature of the population, HIV is rampant and largely unchecked in Mexico border towns adjacent to US cities.

While syringe exchange programs are key, more needs to be done to educate the citizens of both countries:
And with Mexico’s border cities serving as funnels for workers and goods traversing the two countries, Tijuana’s AIDS crisis poses a direct threat to the United States.
“I call HIV the uninvited hitchhiker,” said Steffanie Strathdee, a leading AIDS researcher at the University of California’s Division of International Health and Cross-Cultural Medicine.
A survey by university researchers found that 64 percent of 116 HIV-positive Tijuana residents crossed into the United States at least once a month. Nearly half of men having sex with men in Tijuana and 75 percent of those in San Diego reported having partners across the border. And of 1,000 prostitutes interviewed in Tijuana, 69 percent had U.S. clients who crossed the border for their services.
The federal ban on syringe exchange programs was lifted in the first few weeks of 2016, largely in response to a nationwide heroin and HIV epidemic in America’s heartland. Federal monies cannot be allocated to purchase needles, but cover all other expenses including staff, vehicles, and gas. State and local funding could be used to purchase needles. Still, adoption of programming has been slow.
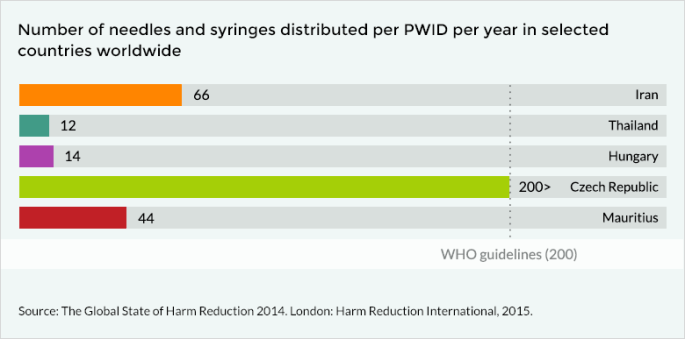
Globally, only 90 needles are available per PWID annually. This is less than half the recommended amount of 200, and many countries provide far fewer.
With a dubious history of HIV prevention and intervention, it is no wonder Russia’s HIV epidemic is increasing 10-15% each year. Recent data show that 1 in 50 people in Russia’s 4th-largest city are HIV-infected. When outside funding for SSPs was withdrawn in 2010 – as Russia was then classified as a high-income country – SSPs dwindled from 80 to 10. Intravenous drug use accounts for 58% of HIV infections.
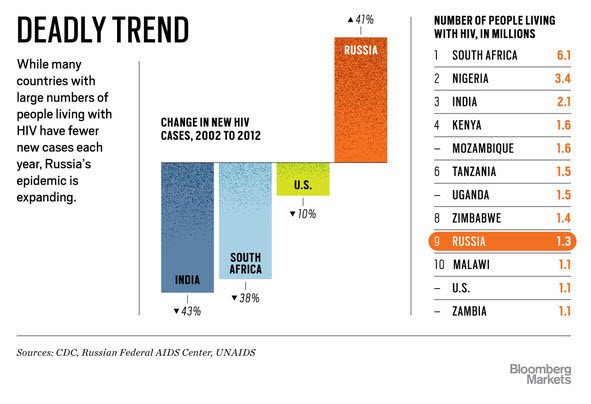
Under Putin’s conservative regime, HIV infections have nearly doubled since 2010 – 500,000 to 930,000 registered carriers – and are projected to reach 3 million (2 million registered carriers) within the next 5 years. Despite annual spending of $418 million (US) rates are increasing as the lion’s share is spent on antiretroviral therapy, not prevention.
President-elect Trump has been surprisingly vocal in praising Putin, and unsurprisingly obtuse about how he plans to address HIV domestically and abroad. When asked whether he would support the President’s Emergency Fund for AIDS Relief, Trump was not un-supportive:
Well, I like committing to all of those things. Those are great things. Alzheimer’s, AIDS, so many different — you now, we are close on some of them. On some of them, honestly, with all of the work that has been done — which hasn’t been enough, we are not very close. But the answer is yes. I believe so strongly in that. And we are going to lead the way.
In perhaps the weirdest twist yet, Vice President-elect Mike Pence could prove to be an ally for continued funding of SSPs in the US. In 2015, an upsurge in HIV infections in Indiana led then-Governor Pence to advocate for syringe exchange programs after a career of staunchly opposing such legislation.
And what of those border states? Perhaps Trump’s fabled wall might come in handy.
