

On February 8, 2019, city councilors in Los Angeles met to approve a resolution declaring LA a “city of sanctuary.” It was hailed as a victory amid growing political tension and derision, a “symbolic welcome sign,” according to Councilman Gil Cedillo, that was supposed to “set the tone for the way we want our residents to be treated.” However, for the 31,285 Angelenos who are experiencing homelessness, Los Angeles is anything but a sanctuary.
You know you’ve stumbled into LA’s Skid Row the moment you arrive. Trash clings to the streets in heaps, stacked haphazardly against rows of tents so densely packed it’s difficult to find the sidewalk. It’s a stark contrast to the dazzling city skyline that frames the neighborhood. This isn’t a part of Los Angeles you can see from the sterile aerial shots that punctuate film and television, but it’s the reality of a county with over 10,000,000 residents and wage growth that can’t keep up with the rising cost of living.
Everyone in Los Angeles, from City Hall to residential streets, agrees that more must be done. Inevitably, however, most attempts to build temporary or permanent supportive housing in Los Angeles is met with public resistance. NIMBY, the acronym for “Not in My Back Yard,” refers to the opposition of development in one’s own neighborhood, even if they would otherwise support such a project somewhere else. NIMBYism is rampant in LA’s complex and powerful network of neighborhood associations and councils. When city officials met with residents of Sherman Oaks, a wealthy neighborhood on the west side of the city, to show proposals for homeless housing projects, residents turned out in force to oppose the plans. One resident went so far as to propose his own solution to the need for emergency shelters in Los Angeles:
“You want me to have compassion for people who don’t care about themselves?…I’m proposing maybe you build a reservation for these homeless somewhere out in the desert…when we interned the Japanese during the Second World War, we didn’t intern them in the city”.
Much of this resentment and stigmatization comes from the deeply held American belief in the “prosperity gospel.” In other words, those who work hard and are free from vices are protected against material scarcity. Homelessness, then, is a personal failing and not a societal one. It’s time we reframe homelessness.
Public officials, public health professionals, and advocates across Los Angeles need to change the way we talk about homelessness to end the rampant NIMBYism in the city. It’s time to adopt a rights-based approach that focuses on the systemic failures that are determinants of homelessness. We need to abandon the “treatment first” approach to combating homelessness, where we attempt to fix the precipitating effects of inadequate housing (substance abuse, mental illness, poor health) before providing stable housing. Instead, programmatic and policy efforts should focus on “housing first” approaches that satisfy basic human needs before attempting to solve complex behavioral and lifestyle issues. The model is evidence-based and, unlike many interventions designed to combat homelessness, it’s effective. Investments in housing first approaches reduced homelessness by 91% in Utah, and research efforts in Seattle show that the savings generated by reducing the need for crisis intervention services more than makes up for the cost of housing first projects.
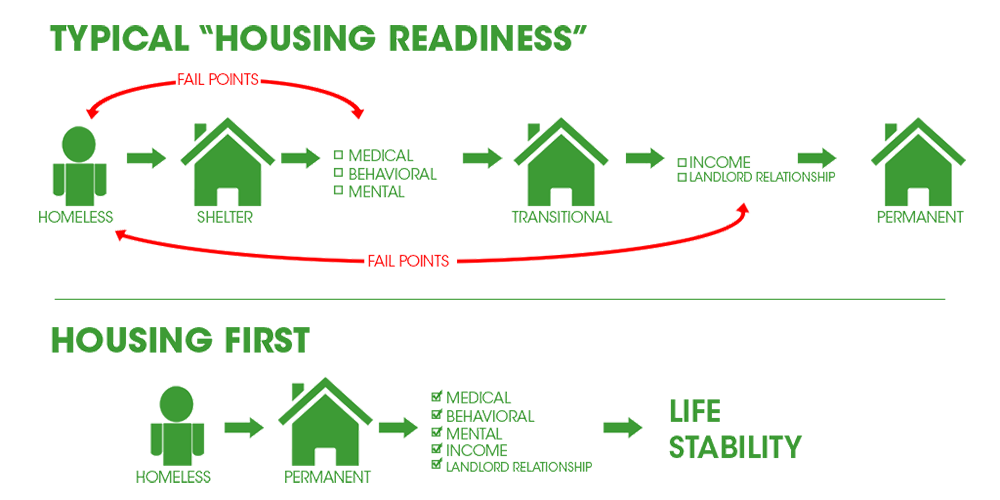
Image Credit: The Spotlight
Los Angeles has the opportunity to lead by example in a world that is growing increasingly less empathetic to the plight of the vulnerable. However, we cannot be the city that birthed the “Me Too” movement and turn away from the fact that half of all women who are homeless report that they are domestic violence survivors. We cannot say that we are a city that believes that black lives matter when we know that while only 8% of LA County identifies as black or African American, they make up over one-third of the unsheltered population. It is unconscionable that our city turns out in force for Pride but fights efforts to house homeless youth, nearly half of whom cite whom they love as the reason they are homeless.
In December, Los Angeles hosted the UN’s celebration of the 70th anniversary of the Universal Declaration of Human Rights, a document that states in no uncertain terms that housing is a right of every person everywhere. If we are to be taken seriously in our defiance of increasingly discriminatory national rhetoric, we must do better here at home.
“Everyone has the right to a standard of living adequate for the health and well-being of himself and of his family, including food, clothing, housing and medical care and necessary social services, and the right to security in the event of unemployment, sickness, disability, widowhood, old age or other lack of livelihood in circumstances beyond his control.“
-UDHR, Article 25.1
Read more about evidence based messaging campaigns around homelessness.
