


Today, September 29, marks World Heart Day (WHD) around the world. World Heart Day brings awareness to the prevention and control of cardiovascular diseases (CVDs) which plays a significant role in our daily lives contributing to our overall health and wellness.
What are Cardiovascular diseases?
Cardiovascular diseases are a group of disorders of the heart and blood vessels and they include:
- Coronary heart disease – disease of the blood vessels supplying the heart muscle;
- Cerebrovascular disease – disease of the blood vessels supplying the brain;
- Peripheral arterial disease – disease of blood vessels supplying the arms and legs;
- Rheumatic heart disease – damage to the heart muscle and heart valves from rheumatic fever, caused by streptococcal bacteria;
- Congenital heart disease – malformations of heart structure existing at birth;
- Deep vein thrombosis and pulmonary embolism – blood clots in the leg veins, which can dislodge and move to the heart and lungs.
According to the World Health Organization (WHO), cardiovascular diseases take the lives of 17.7 million people every year, and accounts for 31% of all global deaths. Of these deaths, 85% are due to heart attack and stroke.
Projects around the world
The global fight against CVDs is happening throughout the world. Some examples include:
– Through the HEARTS project based in Manila, Philippines, WHO and partners like the United States Centers for Disease Control and Prevention (CDC), are supporting ways to fight cardiovascular disease through training, planning and implemention.
– A two-year Standardized Hypertension Treatment project launched in 2015 by the Pan American Health Organization (PAHO) and CDC on the Caribbean island of Barbados, enacted a mission to improve hypertension treatment and control among Barbadians with raised blood pressure through standardizing care for hypertensive patients, prescribing and making available the most effective medicines for treating each person’s condition. The principal investigator of the project highlighted, “It was also encouraging to see the cultural and behavioural change in the clinics among health workers who had to deliver a more focused form of care.” It is important to also note how cultural and social factors play a vital role to behavioral change when it came to seeing patients achieving satisfactory blood pressure control.
Specific intervention activities included: (1) Developing salt reduction and tobacco control plans, (2) Implementing simplified and standardized management protocols, (3) Improving access to medicines and technologies, and (4) Building capacities of health and other providers.
http://www.who.int/news-room/feature-stories/detail/treating-cardiovascular-disease-in-barbados
Key messages to protect heart health
There are small, yet very impactful ways to make “heart health at the heart of all health”. Here are some facts/tips!
- Tobacco use, an unhealthy diet, and physical inativity increase the risk of heart attacks and strokes.
- Engaging in physical activity for at least 30 minutes every day of the week will help to prevent heart attacks and strokes.
- Eating at least five servings of fruit and vegetables a day, and limiting your salt intake to less than one teaspoon a day, also helps to prevent heart attacks and strokes.
When it comes to reducing cardiovascular diseases and improving heart health, it is pivotal to identify those individuals with or at highest risk of CVDs due to risk factors such as hypertension, diabetes, hyperlipidaemia or an already established disease to ensure they receive appropriate treatment in order to prevent premature deaths. During 2015, 17 million premature deaths occurred from noncommunicable diseases (under the age of 70) with 82% of deaths reported in low- and middle-income countries, and 37% caused by CVDs (WHO, 2017). Although there has been great strides toward the prevention of cardiovascular diseases, inequalities including access to noncommunicable disease medicines, and basic health technologies in all primary health care facilities is essential to those in need of receiving treatment and education.
The epidemic of cardiovascular diseases has also impacted my life with my grandmother,mother, and all 4 of my aunts and uncles suffering from hypertension. In March 2018, my cousin at the age of 35 suffered from a massive stroke and is successfully recovering. I spent bringing awareness to this day by cooking popular caribbean dishes with a healthy spin and educating family and friends across the United States and Caribbean on the importance of having and maintaining a healthy heart. In addition, I took a 2 mile walk through my neighborhood taking in the beautiful Florida scenery and cool breeze.
How did you celebrate World Heart Day?
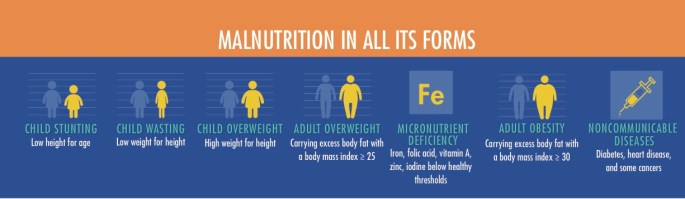 Image Source: Global Nutrition Report 2016, p 21.
Image Source: Global Nutrition Report 2016, p 21.

