In response to an online petition, Dr. Amy Hagopian, our Section’s Nominations Committee Chair, received the below thoughtful reply from her Congressman, Adam Smith (D-WA). The petition asked that U.S. welcome refugees from Syria, despite opposition from xenophobic governors around the country. Here’s a link to a petition YOU can sign!
Dear Amy,
Thank you for contacting me with your concerns regarding the situation in Syria. I appreciate hearing your thoughts on this important issue.
The civil war in Syria is a highly complex struggle between Bashar al-Assad’s authoritarian regime and the fragmented groups that oppose it. As the conflict in Syria has become more violent and protracted, radical elements that directly and seriously threaten our and our allies’ security have become more powerful. It has also become an enormous humanitarian catastrophe. Since the unrest and violence began in 2011, the number of Syrians seeking refuge in neighboring countries or Europe has increased above 4 million. The United Nations Refugee Agency reports that 12.2 million people inside Syria have been affected by the conflict, with nearly 7.6 million displaced internally.
The tragic terrorist attacks in Paris have complicated the situation even further. Our number one priority must be protecting the United States and the American people from terrorist attacks. In the strongest possible terms, I condemn the cowardly attacks in Paris and send my deepest sympathies to the victims. I also welcome the French government’s increased efforts to combat terrorists in Syria. It is important that as we fight terrorism, we must stay true to the values enshrined in our Constitution, remember that we are a nation of immigrants, and not let terrorist groups define or change who we are.
Amidst the conflict, radical groups – like Jabhat al Nusra and the Islamic State of Iraq and Syria (ISIS) – have established safe havens and where, they have attracted substantial financial resources. The strongest and most violent group, ISIS, has continued a campaign of terror and has launched violent and deadly attacks in Northern and Western Iraq. ISIS victories over the Iraqi armed forces have made them a real and dangerous threat to the government in Baghdad and the region. Additionally, the civil war in Syria has attracted a large number of foreign fighters, including from Europe, many of whom are fighting with forces affiliated with ISIS or al Qaeda. As we have seen, these foreign fighters may eventually return to their home countries or go to others where their new combat skills and increased radicalization can be used to subvert other governments.
The civil war in Syria has devolved into a protracted conflict that is dangerously destabilizing. The increasing flows of refugees to neighboring countries place a real strain on already over-burdened public services. Sectarian tensions are on the rise and can lead to further displacement of refugees as host communities become increasingly frustrated with the length of their stay. The humanitarian crisis is quickly shifting from being a consequence of the Syrian conflict to being a potential driver of conflict itself, threatening regional stability. Additionally, the increased activity of Hezbollah, the Iranian-allied militia within Lebanon, and its involvement in the Syrian conflict has escalated tensions between Lebanon and Israel, presenting a great security risk.
The United States has not turned a blind eye to the hurt and suffering of the Syrian people and has been the largest contributor of humanitarian assistance to the crisis, providing over $4.1 billion between Fiscal Years 2012 and 2015. These funds have been used to provide critical, lifesaving services for internally displaced populations within Syria and refugees in neighboring countries, including Jordan, Iraq, Lebanon, Turkey, and Egypt. Channeled through United Nations (UN) agencies and non-governmental organizations, U.S. emergency assistance provides Syrian families with food, medical care and supplies, shelter, and funding for water, sanitation, and hygiene projects.
Due to the worsening refugee situation and immediate need for increased assistance, on July 31, 2015, the U.S. Agency of International Development (USAID) announced an additional $65 million in emergency food assistance. These funds are for the UN World Food Program (WFP), which serves approximately 4 million people inside Syria and 1.6 million refugees in neighboring countries every month.
To help address the refugee crisis, I have taken a number of steps. I supported increased funding for refugee-related program in Fiscal Year 2016 so that resettlement agencies have the resources necessary to help these refugees. I believe that helping our partners in the region and European allies cope with this stressful and destabilizing situation is in our national interest and ultimately helps keep this crisis from devolving into further chaos. I also joined a letter to Secretary of State John Kerry and Secretary of Homeland Security Johnson asking them to increase the number of people eligible to apply for refugee status. I have also called for the Department of State and Homeland Security (DHS) to improve coordination of the lengthy security check process for those applying for asylum, as well as informing families when some but not all of their members have been cleared. Finally, I have joined other members in advocating for the U.S. to increase the number of refugees we are admitting through our resettlement program from 70,000 to 85,000 per year.
To date, of the millions of law-abiding Syrian refugees, less than 1,800 have been resettled in the United States. Applicants for refugee status are held to the highest level of security screening through which we evaluate travelers or immigrants to the United States. If as a result of the security process, U.S. security agencies cannot verify details of a potential refugee’s story to that agency’s satisfaction, that individual cannot enter the United States. I will continue to pursue ways to make sure our vetting process is effective, without unduly burdening bona fide refugees fleeing the terrible situation in Syria and Iraq.
To be very clear, the United States thoroughly vets all refugees. Refugees are subjected to an in-depth interagency vetting process that includes health checks, verifications of biometric information to confirm identity, and multiple layers of biographical and background checks. Moreover, applicants get interviewed in-person. Members of the interagency team includes the FBI’s Terrorist Screening Center, the State Department, DHS, the National Counterterrorism Center, and the Department of Defense. The background check process takes between 18-24 months, happens before an application is approved; and occurs long before a refugee would be able to enter the United States.
The American SAFE Act of 2015, H.R. 4038, which was brought to the House floor for a vote by House Republicans on November 19, 2015, would effectively shut down resettlement of refugees from the Syria and Iraq region. It is wrong to deny asylum to refugees on the basis of inaccurate assumptions, fear, and prejudice, and that is why I voted against it. We must continue to stand strong as an international community and remember that refugees are fleeing terrible conditions and persecution. As we move forward, let us unite to use the tools at our disposal – diplomatic, military, intelligence, and development – to defeat extremism and the terrorism it breeds.
I have also heard several concerns regarding U.S. military involvement in Syria. I am acutely aware of the great cost we incur in both blood and treasure when we ask our men and women in uniform to secure our interests abroad. I share your concerns about becoming militarily involved in another costly conflict in the Middle East. Any consideration of the use of U.S. military force is not one to be taken lightly – especially considering our experiences in Iraq and Afghanistan and the limited ability to affect certain outcomes in those countries. Ultimately, this is a fight between the Syrian people about who will control the future of their country.
The best way to protect ourselves and our allies in the region from the chaos in Syria is by building the Syrian moderate opposition’s capacity so they can stand their ground and fight this war. There is no easy way to identify those elements in the opposition that we can work with, although we have some developed some local allies, such as the Iraqi and Syrian Kurds and some local Sunni allies and are working to identify additional such forces that we can support. By helping those who are fighting ISIL, the U.S. can ensure moderate elements have a chance at playing a role in the creation of an inclusive transitional government, if a peace deal were to be reached in the future.
Due to the extremely concerning developments in Syria and Iraq, the President has taken a number of actions. First, the United States has conducted literally thousands of airstrikes intended to degrade ISIS in Syria and Iraq, reduce their ability to raise money, and to support the local allies we have identified. We are also currently retraining and equipping a number of brigades in the Iraqi Army and Congress has provided over $1 billion for this process. The President also decided that training and equipping moderate elements of the opposition was necessary in Syria. On June 26, 2014, he requested $500 million as part of a supplement to the budget request known as “overseas contingency operations.” These funds would be used to train and equip vetted elements of the Syrian armed opposition to help then fight against the Assad regime. As you may know, this training program did not meet expectations nor objectives and the training portion has been suspended. Since that time, however, the approach has transitioned to equipping moderate elements in hopes of empowering them in this fluid situation, and the President has announced that fewer than 50 U.S. Special Forces will be deployed to Syria to help accomplish this goal. I will continue to monitor developments in the region, understanding that there are always risks involved in conflict and I do not take them lightly.
Moreover, I support the Obama Administration’s diplomatic efforts to find a political solution to the situation in Syria that respects the rights of people. While those efforts have not yet produced any sort of agreement that would lead to an end of the war in Syria, I believe that it is helpful to have the major international countries that are involved in the conflict in Syria discussing possible ways to bring about a political transition and end to the civil war. Hopefully, such a course forward would also address the underlying causes of the refugee crisis. Until a solution can be found, we must continue to help those seeking refuge. We cannot let what happened in Paris cloud our judgement, drive policy or destroy the fabric of what America stands for. We need to be strong and smart to fight terrorism. If we turn our backs on refugees, then we risk making ISIS stronger.
Again, thank you for contacting me with your concerns regarding these important issues.. Rest assured that I will closely follow the continuing developments as they arise. Should you have any additional questions or concerns, please do not hesitate to contact me again.
Sincerely,
Adam Smith
Member of Congress


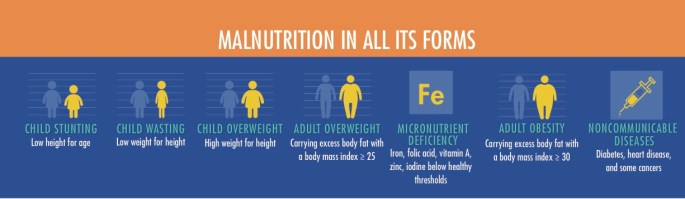 Image Source: Global Nutrition Report 2016, p 21.
Image Source: Global Nutrition Report 2016, p 21.
